VN
Dự đoán và lập kế hoạch điều trị chỉnh nha trên phim sọ mặt nghiêng dựa trên bằng chứng y học
1. Tổng quan về dự đoán và lập kế hoạch điều trị chỉnh nha trên phịm sọ mặt nghiêng
Lập kế hoạch điều trị đóng một vai trò quan trọng trong việc đạt được kết quả điều trị chỉnh nha tối ưu. Việc lập kế hoạch điều trị được cá nhân hóa và không cần phải tuân theo “các tiêu chuẩn giải phẫu nghiêm ngặt về khớp cắn và hình dạng khuôn mặt”.1 Phân tích phim sọ mặt nghiêng là một công cụ thiết yếu dùng để chẩn đoán và hỗ trợ lập kế hoạch điều trị.2,3
Đọc thêm về:“Phân tích phim đo sọ từ xa theo Ricketts”.
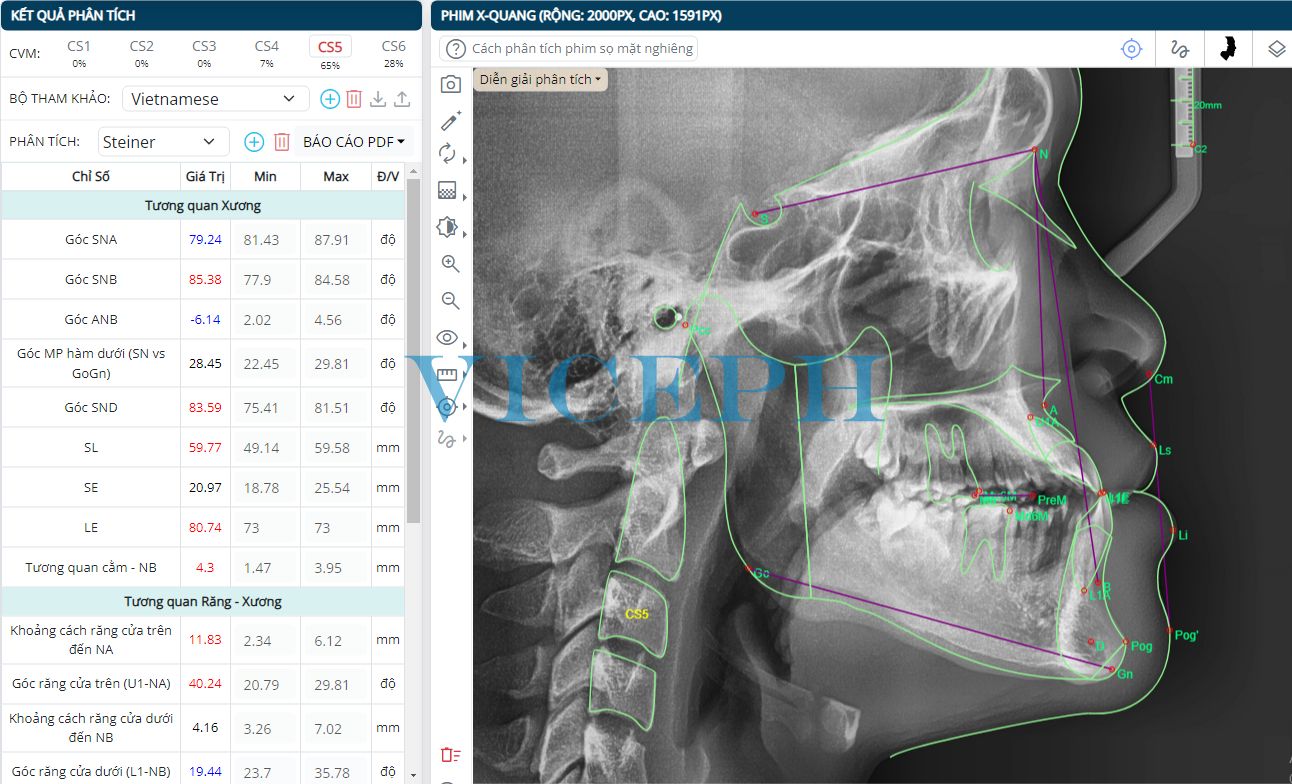
Hình 1. Phân tích phim sọ mặt nghiêng hỗ trợ lập kế hoạch điều trị chỉnh nha.
Cụ thể hoá mục tiêu điều trị – Visualized Treatment Objective (VTO) với phim sọ mặt nghiêng và ảnh mặt nghiêng được sử dụng để hỗ trợ lập kế hoạch điều trị. VTO được sử dụng như một công cụ để dự đoán đặc điểm mô mềm đáp ứng với điều trị chỉnh nha, đưa ra hình ảnh dự đoán có thể xảy ra nhất, cho phép bác sĩ lâm sàng hình dung dễ dàng hơn hiệu quả của các phương án điều trị khác nhau. VTO cũng thường được sử dụng như một “bản thiết kế” để từ đó đưa ra trình tự điều trị.4
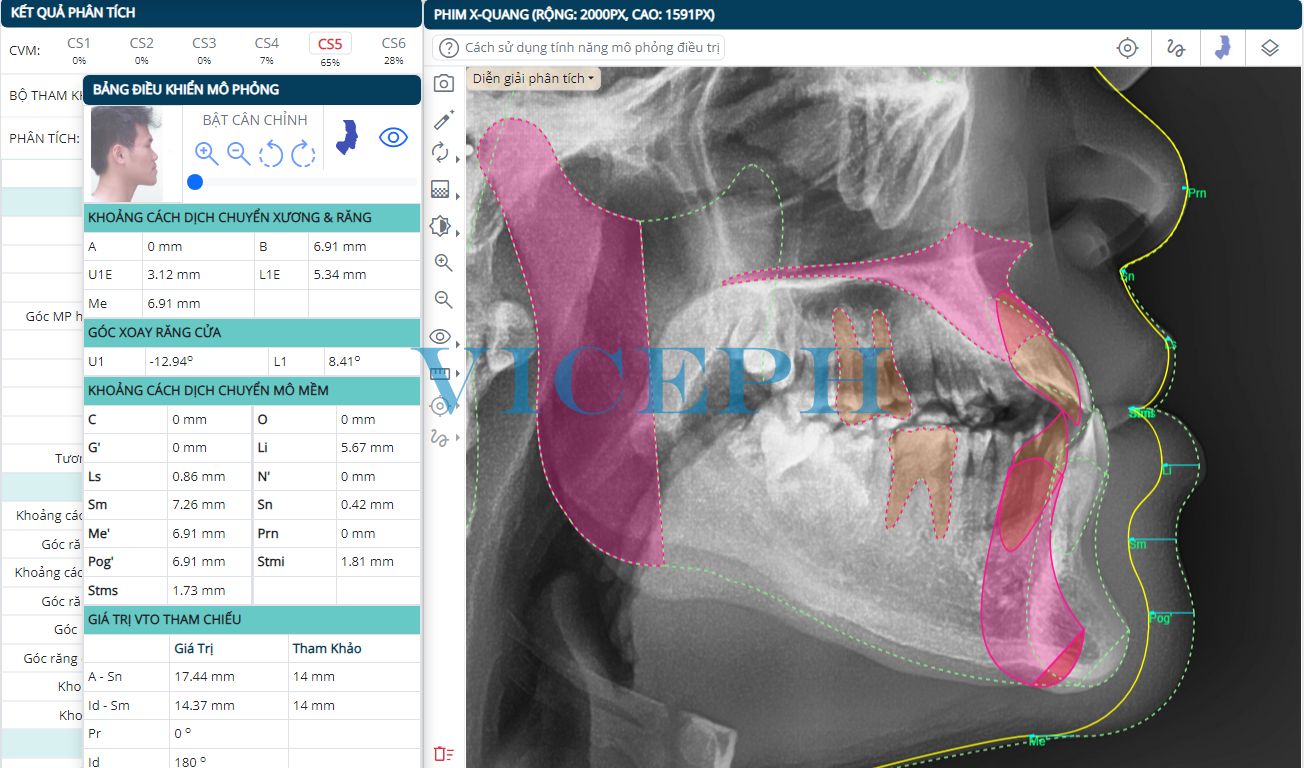
Hình 2. Công cụ VTO – cụ thể hoá mục tiêu điều trị sử dụng phim sọ mặt nghiêng trên Viceph.net.
Cụ thể hoá mục tiêu điều trị (VTO) sử dụng phim sọ mặt nghiêng đã được nhiều tác giả đề xuất, bao gồm phương pháp Jacobson và Sadowsky, phân tích Holdaway và Ricketts cùng những phương pháp khác được đưa vào ứng dụng trong nhiều năm trở lại đây.
Vị trí mô mềm phụ thuộc chủ yếu vào vị trí của mô cứng mà nó phủ lên, bao gồm xương và răng. Chính vì vậy, để dự đoán sự thay đổi của mô mềm sau quá trình điều trị, ta cần dựa trên sự dịch chuyển xương và răng trong kế hoạch điều trị.
2. Dịch chuyển mô mềm khi dịch chuyển răng (Holdaway)
Dịch chuyển răng là dịch chuyển không thể thiếu trong chỉnh nha, và dịch chuyển mô mềm do dịch chuyển răng là thường gặp.
Năm 1983, Reed A. Holdaway đã trình bày một phân tích mô mềm trên phim sọ mặt nghiêng đồng thời chỉ ra sự dịch chuyển của mô mềm khi dịch chuyển răng dựa trên nhiều năm quan sát và mô tả bệnh nhân từ quá trình thực hiện lâm sàng.
Các phát hiện này chỉ ra rằng, nói chung, đối với thanh thiếu niên, độ dày bình thường của mô mềm tại điểm A là 14 đến 16mm. Vì điểm A có thể bị thay đổi do chuyển động của răng, headgear,…, mô mềm sẽ đi theo điểm này và giữ nguyên độ dày. Trong các trường hợp môi có độ dày bình thường, người ta quan tâm đến độ thuôn của môi, được tính bằng hiệu độ dày mô mềm tại điểm A và độ dày mô mềm ở làn môi đỏ quan sát được trên phim sọ mặt nghiêng.5
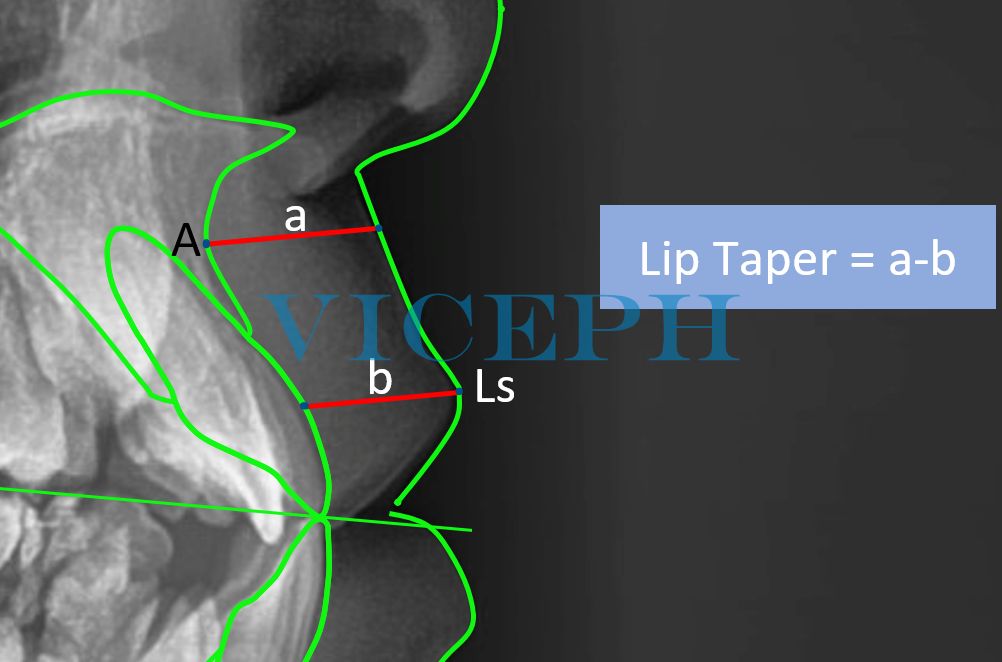
Hình 3. Độ thuôn của môi trong phân tích mô mềm – Holdaway.
Khi môi trên có độ thuôn lớn như trong trường hợp răng quá nhô, mô mềm sẽ dày lên khi các răng cửa được di chuyển về phía lưỡi cho đến khi mô đạt đến độ dày tại điểm A (trong vòng 1 mm độ dày tại điểm A). Khi độ thuôn môi đã được loại bỏ, sự di chuyển về phía trong hơn nữa của răng cửa sẽ khiến môi đi theo răng cửa theo tỷ lệ 1:1.5
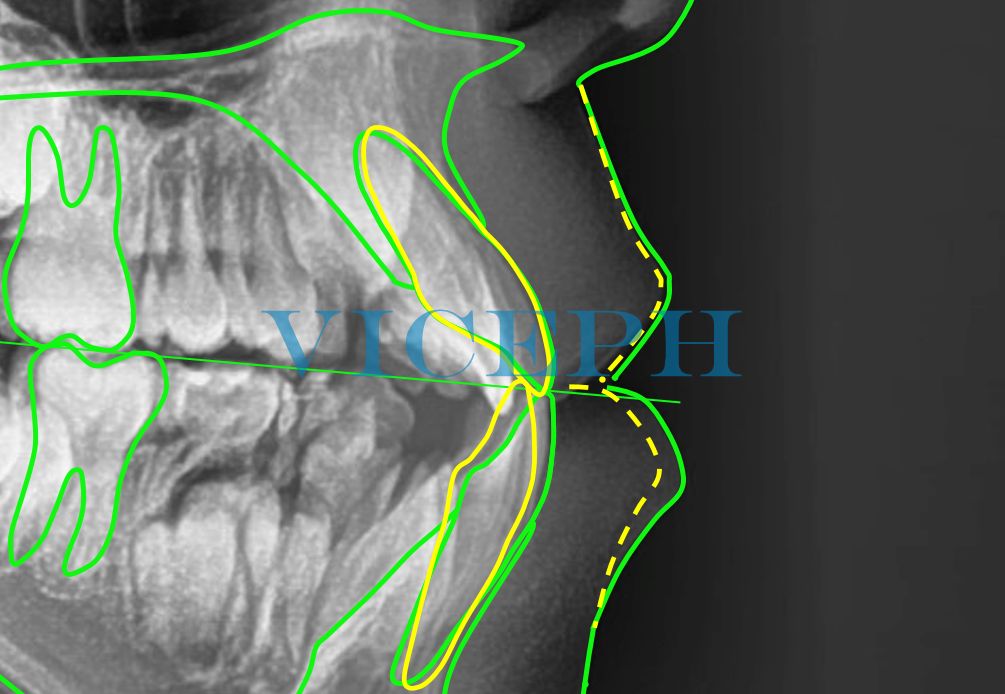
Hình 4. Mô phỏng dịch chuyển mô mềm với tỉ lệ 1:1 ở bệnh nhân có độ dày mô mềm tại điểm A bình thường và độ thuôn môi nhỏ (Lip Taper < 1mm).
Một số trường hợp ngoại lệ như sau: Nếu độ dày mô ở điểm A rất mỏng (ví dụ: 9 đến 10mm), môi có thể di chuyển theo răng cửa ngay lập tức mà vẫn giữ được độ thuôn, bất kể độ thuôn môi nào.
Nếu mô ở điểm A rất dày (ví dụ: 18 đến 20mm), môi có thể không tuân theo chuyển động của răng cửa.
Phản ứng mô của người trưởng thành cũng tương tự như ngoại lệ đầu tiên. Dù có thể có hiện tượng thuôn môi nhưng thông thường môi sẽ theo răng ngay lập tức.
3. Dịch chuyển mô mềm khi dịch chuyển xương (Sugawara)
Dịch chuyển xương trong chỉnh hình răng mặt ít gặp hơn rất nhiều so dịch chuyển răng nhưng lại mang lại thay đổi rất lớn về mô mềm cũng như mặt nghiêng cho bệnh nhân.
Nghiên cứu của Sugawara trên 115 bệnh nhân phẫu thuật chỉnh hình đưa ra công thức thay đổi mô mềm theo dịch chuyển xương. Theo đó, sự đáp ứng của mô mềm phụ thuộc cả vào lượng và hướng dịch chuyển của xương.6 Do đó, ta cần xác định góc giữa vector dịch chuyển của các điểm mào xương ổ răng và mặt phẳng Frankfort; góc này mang giá trị dương khi vector dịch chuyển hướng lên trên, mang giá trị âm khi vector dịch chuyển hướng xuống dưới.
Hình 5. Góc giữa vector dịch chuyển của mào xương ổ răng và mặt phẳng Frankfort.
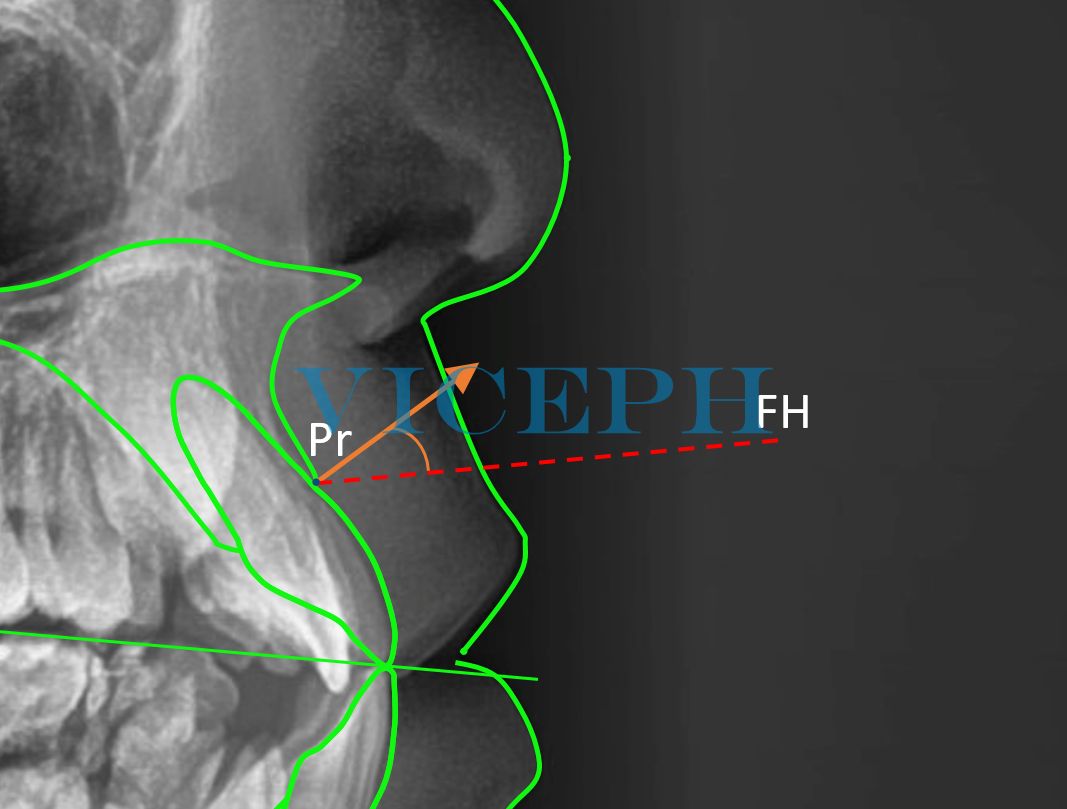
Đối với phẫu thuật xương hàm trên, ta xác định góc dịch chuyển của Pr (Pr Angle). Pr Angle là góc giữa vector dịch chuyển điểm Pr so với vector Po-Or (mặt phẳng ngang Frankfort), gợi ý hướng chuyển động của mô mềm dựa theo chuyển động của xương hàm trên.
Khi dịch chuyển xương hàm trên lên trên và ra trước, mô mềm môi trên và đỉnh mũi dịch chuyển cả lên trên và ra trước.
 Khi dịch chuyển xương hàm trên ra trước, mô mềm môi trên và đỉnh mũi dịch chuyển chủ yếu ra trước, ít dịch chuyển theo chiều dọc.
Khi dịch chuyển xương hàm trên ra trước, mô mềm môi trên và đỉnh mũi dịch chuyển chủ yếu ra trước, ít dịch chuyển theo chiều dọc.
Khi dịch chuyển xương hàm trên xuống dưới và ra trước, mô mềm môi trên và đỉnh mũi dịch chuyển cả xuống dưới và ra trước.
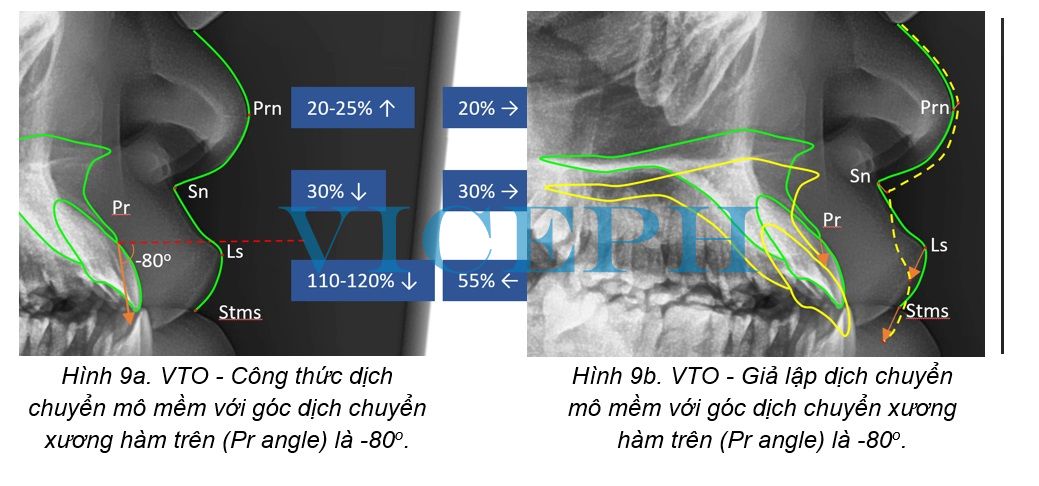
Khi dịch chuyển xương hàm trên xuống dưới, mô mềm môi trên và đỉnh mũi dịch chuyển chủ yếu xuống dưới, ít dịch chuyển theo chiều ngang.
Đối với phẫu thuật xương hàm dưới, ta xác định góc dịch chuyển của Id (Id Angle). Id Angle là góc giữa vector dịch chuyển điểm Id so với vector Po-Or (mặt phẳng ngang Frankfort), gợi ý hướng chuyển động của mô mềm dựa theo chuyển động của thân xương hàm dưới.
Khi dịch chuyển xương hàm dưới lên trên và ra sau, mô mềm môi dưới và vùng cằm dịch chuyển cả lên trên và ra sau.
Khi dịch chuyển xương hàm dưới ra sau, mô mềm môi dưới và vùng cằm dịch chuyển chủ yếu ra sau, ít dịch chuyển theo chiều dọc.
4. Kết luận
Cụ thể hoá mục tiêu điều trị – Visualized Treatment Objective (VTO) giúp các bác sĩ lâm sàng có cái nhìn trực quan về kết quả điều trị dự đoán của các phương án điều trị khác nhau.
Khi VTO được phát triển trong các phần mềm máy tính hiện đại, một công cụ tiện ích ra đời cho phép ta thực hiện nhanh chóng các giả lập kết quả điều trị, giúp ta có thêm nhiều gợi ý để cân nhắc khi lựa chọn kế hoạch điều trị tối ưu.
EN
Predicting and planning orthodontic treatment for correction of tilted facial profile based on medical evidence
1. Overview
Treatment planning plays a crucial role in achieving optimal orthodontic treatment outcomes. The treatment planning process is individualized and does not necessarily have to adhere to ‘strict anatomical standards for occlusion and facial shape’.1 Analysis of tilted skull films is an essential tool used for diagnosis and supporting treatment planning.2,3
Figure 1. Analysis of tilted skull films supporting orthodontic treatment planning
Visualized Treatment Objective (VTO) is used to visualize the treatment goals and support treatment planning. VTO serves as a tool to predict soft tissue responses to orthodontic treatment, providing a visual representation of the potential outcomes and allowing doctors to better visualize the effectiveness of different treatment options. VTO is often used as a “design prototype” to establish the treatment sequence.4
Figure 2. VTO in ViCeph.net
The visualization of treatment objectives (VTO) has been proposed by various authors, including the methods of Jacobson and Sadowsky, Holdaway and Ricketts analysis, along with other methods that have been applied in recent years.
The position of soft tissue is predominantly influenced by the position of the underlying hard tissues, including bones and teeth. Therefore, in order to predict the changes in soft tissue following the treatment process, it is necessary to rely on the movements of bones and teeth in the treatment plan.
2. Soft Tissue Displacement with Tooth Movement (Holdaway)
Tooth movement is an essential component of orthodontic treatment, and accompanying soft tissue displacement is commonly observed.
In 1983, Reed A. Holdaway presented a soft tissue analysis based on tilted skull films and described the soft tissue changes associated with tooth movement based on years of clinical observations and patient descriptions.
These findings indicated that, in general, for adolescents, the normal thickness of soft tissue at point A is 14 to 16mm. As point A can be altered by tooth movement, headgear, and other factors, the soft tissue will follow this point and maintain its thickness. In cases where the lip has normal thickness, attention is given to the lip taper, which is determined by the difference in soft tissue thickness at point A and the thickness of the vermilion border of the lip.5
Figure 3. Lip taper in soft tissue analysis – Holdaway
When the upper lip has a larger taper, such as in the case of excessive overjet, the soft tissue will thicken as the incisor teeth are moved lingually until the soft tissue reaches the thickness at point A (within a 1mm range of thickness at point A). Once the lip taper is eliminated, further lingual movement of the incisor teeth will cause the lip to follow the incisors at a ratio of 1:1.5
Figure 4. Simulation of soft tissue displacement with a 1:1 ratio in a patient with normal soft tissue thickness at point A and small lip taper (Lip Taper < 1mm)
Some exceptional cases are as follows: If the soft tissue thickness at point A is very thin (e.g., 9 to 10mm), the lip may immediately move with the incisor teeth while maintaining the taper, regardless of the initial degree.
If the soft tissue at point A is very thick (e.g., 18 to 20mm), the lip may not follow the movement of the incisor teeth.
The soft tissue response in adults is generally similar to the first exceptional case. Although there may be lip taper, the lip typically immediately follows the incisors.
3. Soft Tissue Displacement with Bone Movement (Sugawara)
Bone movement in orthodontic and orthognathic treatment is less common than tooth movement but can result in significant changes in soft tissue and facial angulation for patients.
Sugawara’s study on 115 patients who underwent orthognathic surgery provided a formula for predicting soft tissue changes with bone movement. According to the study, the soft tissue response depends on both the magnitude and direction of the bone movement.6 Therefore, it is necessary to determine the angle between the displacement vector of the skeletal reference points and the Frankfort plane. This angle is positive when the displacement vector is directed upward and negative when it is directed downward.
Figure 5. The angle between the displacement vector of the skeletal reference points and the Frankfort plane
For maxillary orthognathic surgery, the displacement angle of the point Pr is determined (Pr Angle). The Pr Angle is the angle between the displacement vector of point Pr and the vector Po-Or (the horizontal plane of the Frankfort plane). It provides an indication of the direction of soft tissue movement based on the movement of the maxillary bone.
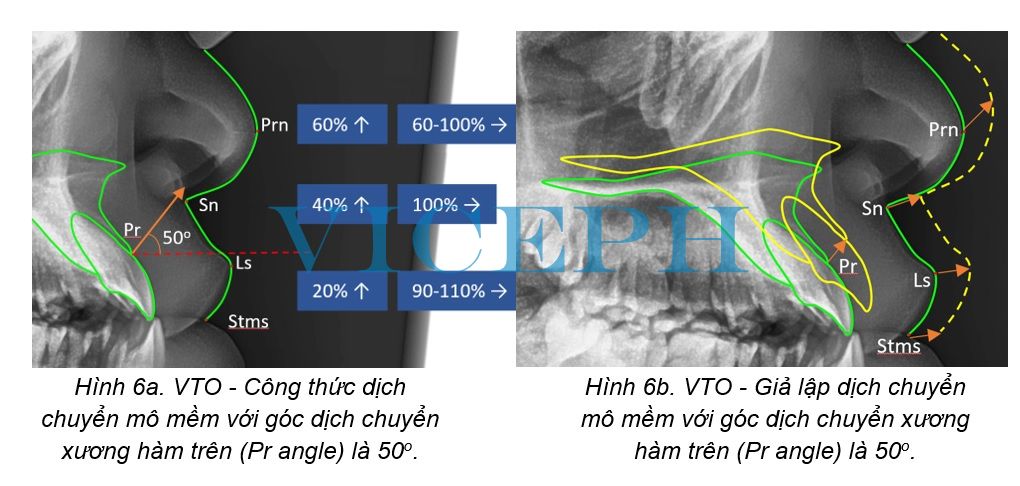
When the maxillary bone is moved upward and forward, the soft tissue of the upper lip and nasal tip also displaces upward and forward.
Figure 6a. VTO - Soft tissue displacement formula with maxillary bone displacement angle (Pr angle) of 50o.
Figure 6b. VTO - Simulate soft tissue movement with the maxillary bone movement angle (Pr angle) being 50o.
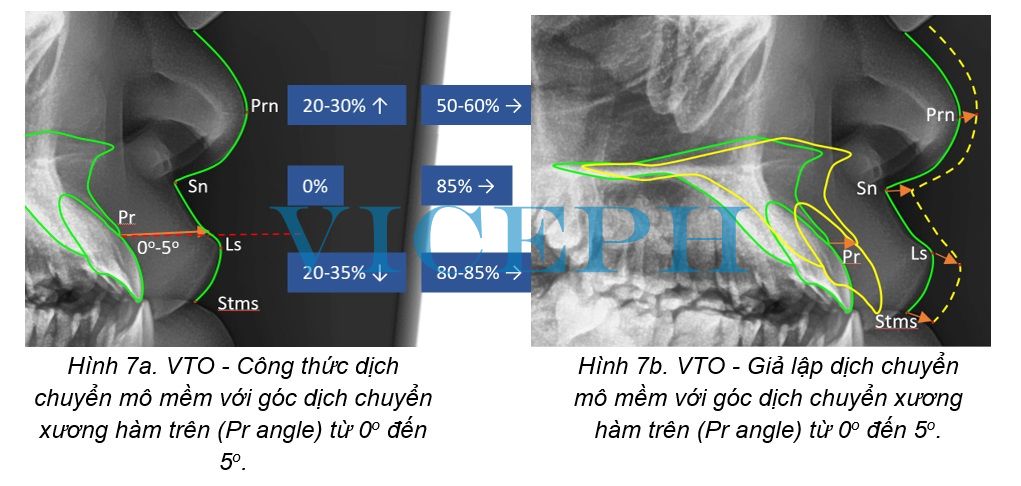
When the maxillary bone is moved forward, the soft tissue of the upper lip and nasal tip primarily displaces forward, with less vertical displacement.
Figure 7a. VTO - Soft tissue displacement formula with maxillary bone displacement angle (Pr angle) from 0o to 5o.
Figure 7b. VTO - Simulate soft tissue movement with maxillary bone movement angle (Pr angle) from 0o to 5o
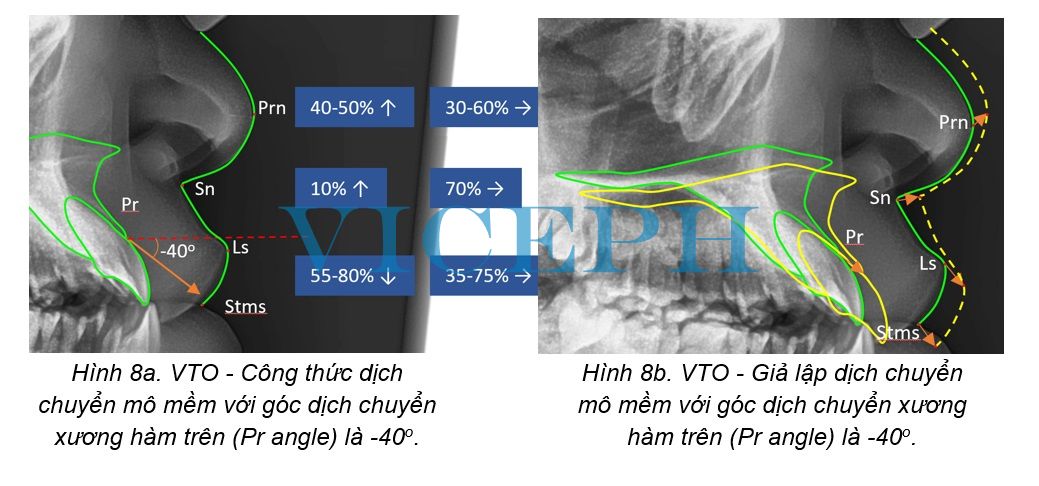
When the maxillary bone is moved downward and forward, the soft tissue of the upper lip and nasal tip displaces both downward and forward.
Figure 8a. VTO - Soft tissue displacement formula with maxillary bone displacement angle (Pr angle) of -40o.
Figure 8b. VTO - Simulate soft tissue movement with the maxillary bone movement angle (Pr angle) being -40o
When the maxilla is moved downward, the soft tissue of the upper lip and nasal tip primarily moves downward, with minimal horizontal movement.
Figure 9a. VTO - Soft tissue displacement formula with maxillary bone displacement angle (Pr angle) of -80o.
Figure 9b. VTO - Simulate soft tissue movement with the maxillary bone movement angle (Pr angle) being -80o
For mandibular orthognathic surgery, the displacement angle of the point Id is determined (Id Angle). The Id Angle is the angle between the displacement vector of point Id and the vector Po-Or (the horizontal plane of the Frankfort plane). It provides an indication of the direction of soft tissue movement based on the movement of the mandibular body.
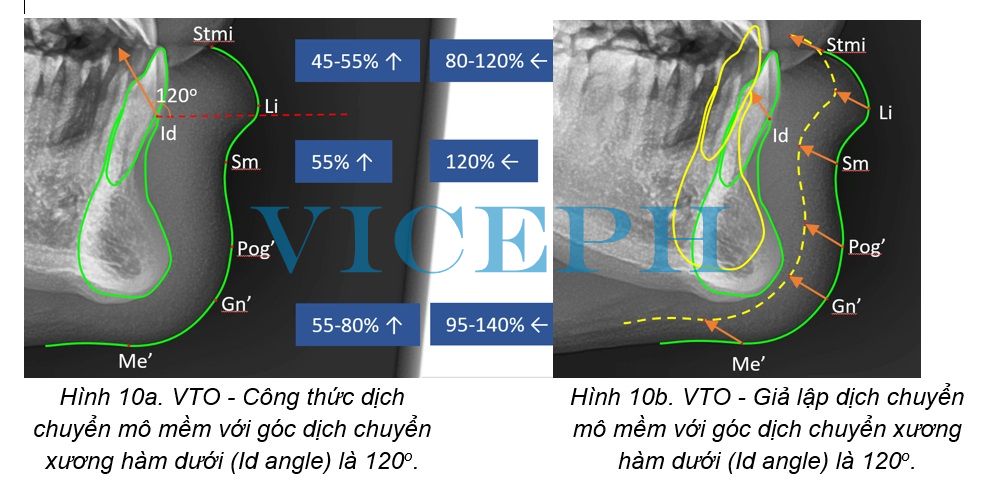
When the mandible is moved upward and backward, the soft tissue of the lower lip and chin area displaces both upward and backward.
Figure 10a. VTO - Soft tissue displacement formula with mandibular displacement angle (Id angle) of 120o.
Figure 10b. VTO - Simulate soft tissue movement with mandibular bone movement angle (Id angle) of 120o.
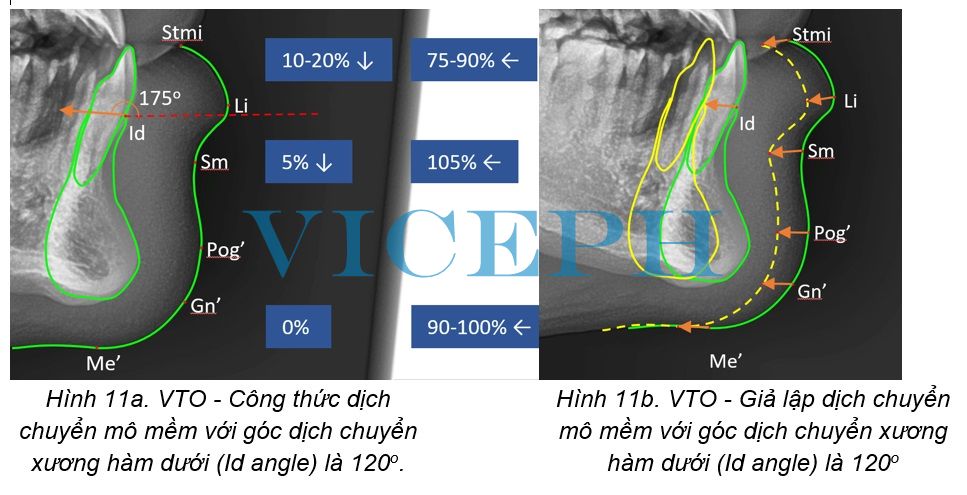
When the mandible is moved backward, the soft tissue of the lower lip and chin area primarily displaces backward, with less vertical displacement.
Figure 11a. VTO - Soft tissue displacement formula with mandibular displacement angle (Id angle) of 120o.
Figure 11b. VTO - Simulate soft tissue movement with mandibular bone movement angle (Id angle) of 120o
4. Conclusion
The visualization of treatment objectives, known as Visualized Treatment Objective (VTO), helps clinicians to have a visual representation of the predicted treatment outcomes for different treatment options.
With the development of VTO in modern computer software, a useful tool has emerged that allows us to quickly simulate treatment results. This provides us with additional insights to consider when selecting the optimal treatment plan.
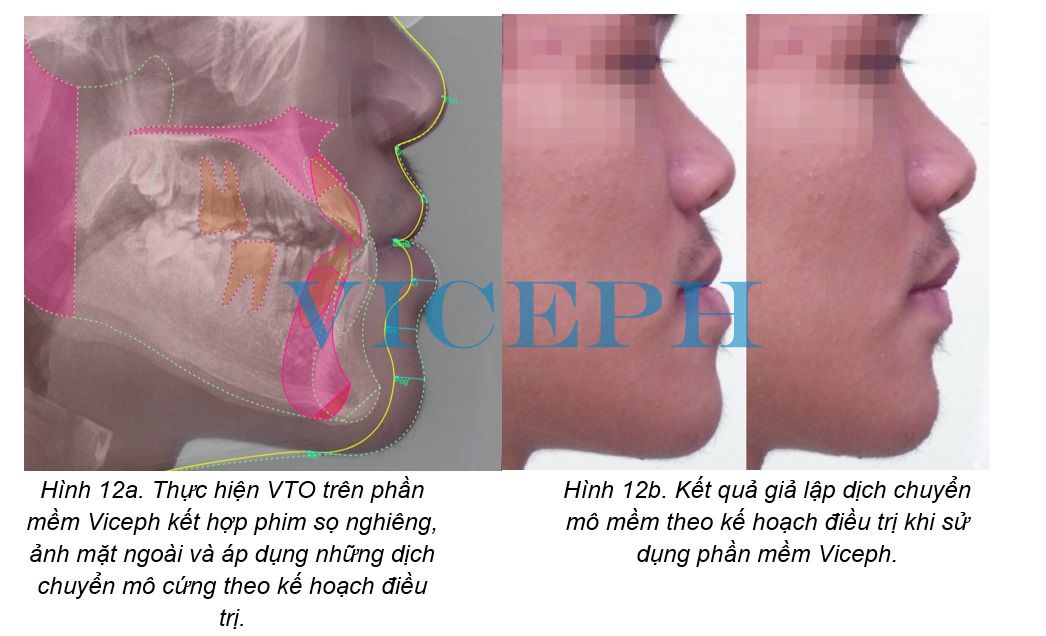
Figure 12a. Perform VTO on Viceph software combining tilted skull films, lateral images and applying hard tissue movements according to the treatment plan.
Figure 12b. Results of simulation of soft tissue movement according to treatment plan when using ViCeph software.
References:
1. Moorrees CFA. Twenty centuries of cephalometry. Radiographic Cephalometry From Basics to 3-D Imaging, 2nd Ed. Chicago: Quintessence Books; 2006: 13-32.
2. Steiner CC. Cephalometrics for you and me. American Journal of Orthodontics. 1953; 39(10): 729-755.
3. Nijkamp P, Habets L, Aartman I, et al. The influence of cephalometrics on orthodontic treatment planning. European Journal of Orthodontics. 2008; 30: 630-635.
4. Thames TL, Sinclair PM, Alexander RG. The accuracy of computerized growth prediction in Class II high angle cases. American Journal of Orthodontics. 1985; 87:398-405.
5. Holdaway RA. A soft-tissue cephalometric analysis and its use in orthodontic treatment planning. Part I. American Journal of Orthodontics. 1983; 84 (1), 1-28.
6. Sugawara J. The theory and practice of modern surgical orthodontic treatment.
Facebook Comments